Key takeaways
- A UAE hospital VMS in 2026 must hold visitor data inside the facility perimeter, align with the federal Personal Data Protection Law (Decree-Law 45/2021), and remain auditable for MoHAP, DoH, DHA and TDRA inspections — sovereign on-premises is the default.
- Six visitor classes drive design: patient visitors under visiting-hours policy, contractors and maintenance staff, medical reps, clinical-trial participants, auditors and inspectors, and medical-tourism patients with carer and family.
- Bilingual English + Arabic with full right-to-left layout is a clinical-safety requirement — a misread badge in a labour-ward corridor is a clinical incident.
- Integration to the clinic management system over HL7 v2 and FHIR R4, plus DICOM viewers and WebRTC for telemedicine carer rooms, replaces the spreadsheet-and-clipboard reception desks still common in mid-tier private hospitals.
- Realistic engagement bands for 2026: Discovery £15k-£40k; Build small £100k-£300k; Build enterprise £400k-£1.4M; per-hospital hardware £20k-£60k; on-premises AI £30k-£90k.
- Fixed-fee phased engagements with weekly demos and a 90-day exit window protect the CFO better than a per-visitor SaaS contract that escalates as the group grows.
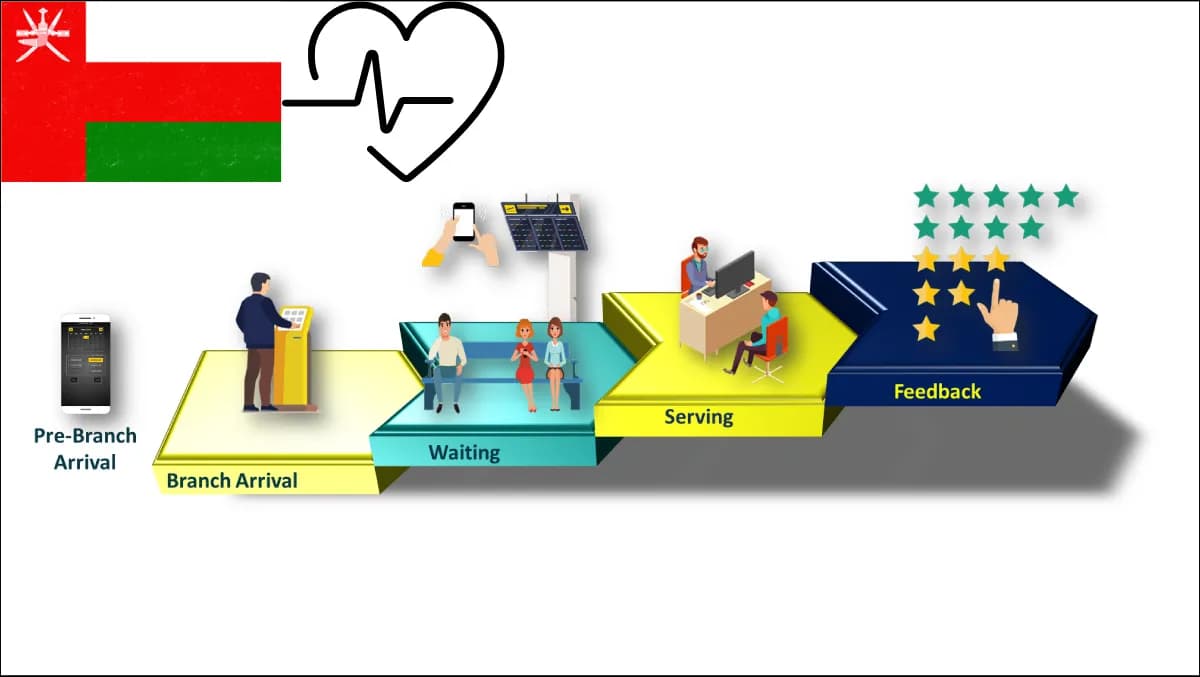
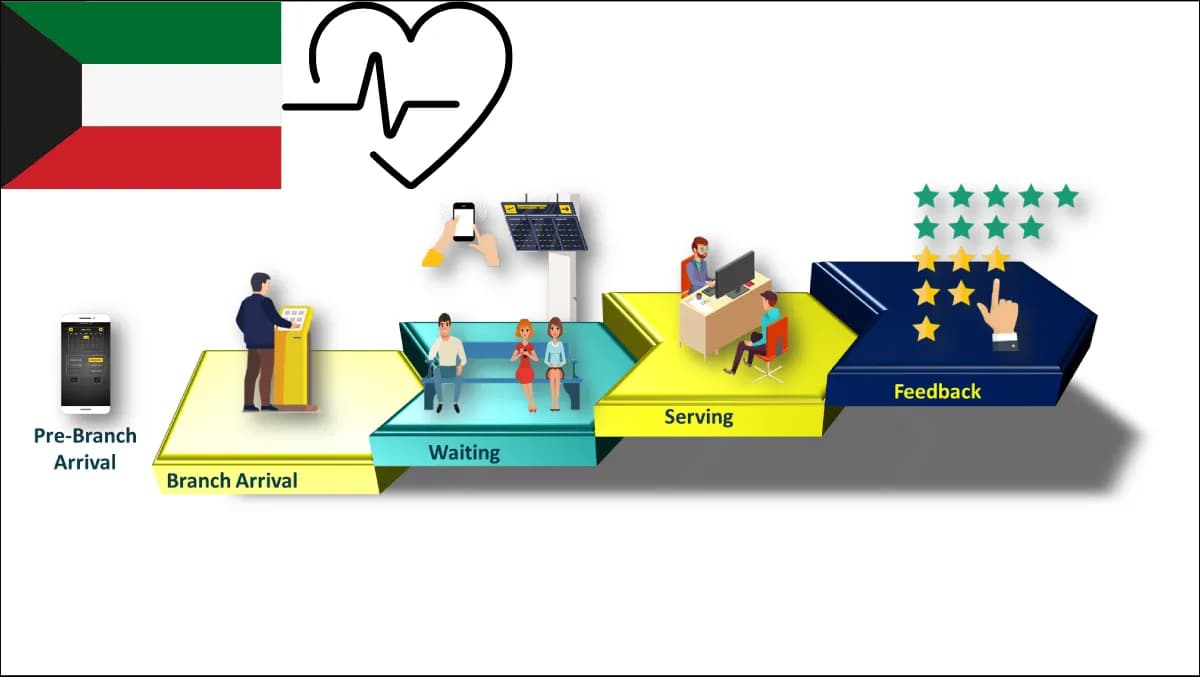
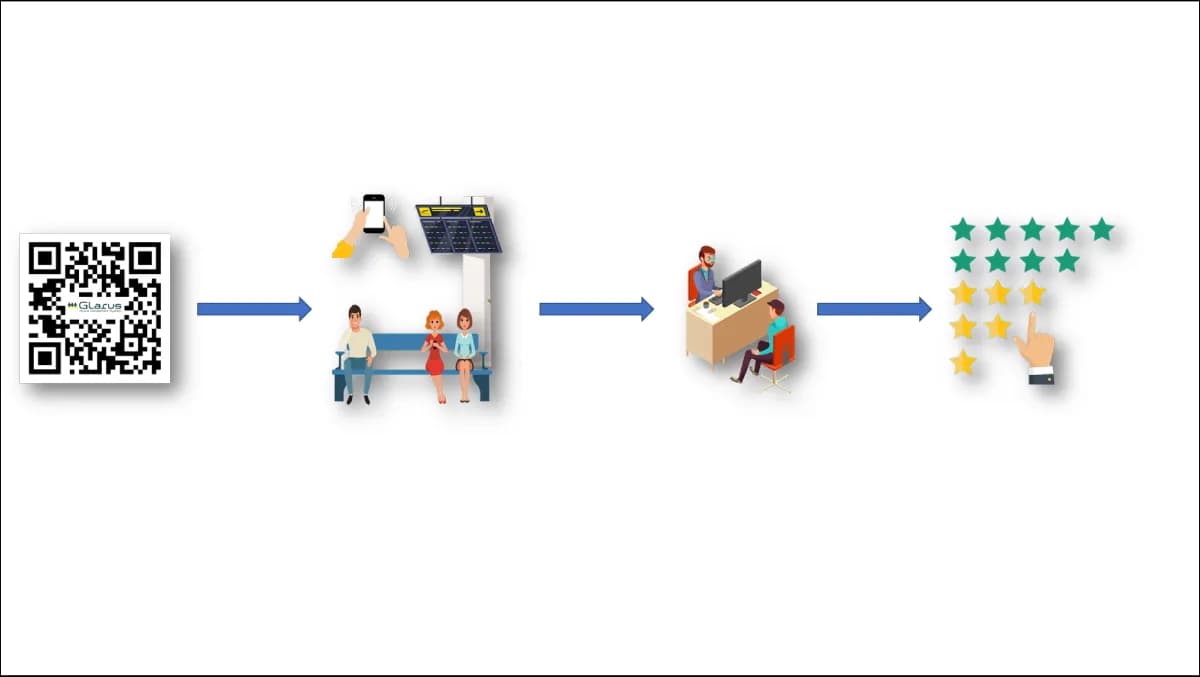
- Hospitals winning the UAE medical-tourism flow are those with a bilingual digital concierge from kerb to consulting room — pre-arrival appointment, kiosk ID, wayfinding to the clinic, visitor management for carer and family, feedback at exit — all on one operator-owned stack.
The UAE healthcare sector has climbed steadily up the value chain since the early 2010s, but most VMS deployments at UAE hospitals were procured before that maturation — single-tenant SaaS portals or paper logs that no longer satisfy the federal Personal Data Protection Law, the emirate health regulators, or the infection-control standards a 2026 JCI surveyor expects. This guide is a senior engineer's playbook for replacing that legacy with a sovereign, bilingual, integrated visitor management system.
Who this guide is for
- Persona 1 — UAE hospital facilities director. You run a 200-600-bed private hospital, handle 600-2,000 visitor movements per day across reception, A&E, maternity, surgical wards and outpatient clinics, and you need a system that distinguishes a patient's spouse from a contractor wheeling oxygen cylinders down the same corridor.
- Persona 2 — infection-control and visitor-policy lead. You write the visiting-hours policy, gate the immunocompromised wards, manage the post-pandemic declaration, and you need a VMS that enforces every policy rather than relying on a receptionist remembering it on a Friday night shift.
- Persona 3 — UAE hospital CISO under federal PDPL plus DHA, DoH and MoHAP rules. You sign off the data-protection impact assessment listing the visitor table as a special-category-adjacent PHI processor, and you need that table to never leave the hospital perimeter.
- Persona 4 — CIO at a multi-site UAE hospital group. You are consolidating four to twelve reception stacks onto one platform with central reporting, federation to the emirate health information exchange, and weekly KPI rollups to the board.
What is visitor management in 2026 — and why it's different for UAE hospitals?
A hospital visitor management system in 2026 is the system of record for every non-staff, non-patient body that crosses the threshold: who they are, who they are visiting, which ward they are cleared for, when they entered and left, their declared health status, and which clinical or security event their movement is later correlated against. It replaces the paper log book, the standalone reception SaaS, and the WhatsApp threads between the security manager and the night shift charge nurse.
A UAE hospital is not an office tower. The visitor mix is heterogeneous — compassionate visitors outside scheduled hours, mothers with children visiting a new sibling, medical reps requesting a consultant slot, contractors with a permit-to-work, clinical-trial participants at a screening, JCI surveyors needing escorted access, MoHAP, DoH or DHA inspectors arriving unannounced, and medical-tourism patients with a carer plus extended family. Visitor records are in scope for the federal Personal Data Protection Law because they combine with a patient's ward to infer condition.
The regulator shape in 2026 is layered. MoHAP sets federal hospital licensing rules. DoH (Department of Health, Abu Dhabi) and DHA (Dubai Health Authority) set emirate-level operational standards including patient and visitor rights, infection control, and data-exchange participation. The federal Personal Data Protection Law (Federal Decree-Law 45/2021) sets controller-processor, consent, cross-border and data-subject-rights obligations across the UAE. TDRA owns the digital identity layer that any visitor-facing app touches. The We the UAE 2031 Health pillar steers the sector toward integrated, citizen-centred care — a fragmented reception contradicts that direction loudly.
The UAE healthcare VMS scoring rubric — 14 criteria
Use these 14 criteria to score every vendor longlisted. No UAE hospital can deprioritise PDPL or bilingual EN+AR.
- 1Sovereign on-premises for PHI-adjacent visitor data. Federal PDPL, MoHAP licensing and emirate health-exchange contracts reward in-perimeter processing. Test: ask for the network diagram showing where the visitor table sits at peak load — if data crosses a public cloud boundary, it is not sovereign on-premises.
- 2Bilingual EN+AR with full RTL at the framework layer. A bilingual baseline is mandatory across UAE healthcare. Test: print a visitor badge with a hyphenated bilingual EN+AR name and a ward code.
- 3Federal Personal Data Protection Law compliance posture. Every UAE hospital has a federal-PDPL DPO who must sign off the visitor-data processing register. Test: ask for the consent-capture screen, data-subject-rights workflow, and retention job — in product, not on a roadmap deck.
- 4HL7 v2 and FHIR R4 integration with the clinic stack. A visitor record that cannot pull "who is in ward 4B" from the clinic management system forces the receptionist to type the patient's name from memory. Test: demonstrate an A04 admit message landing in the VMS within five seconds.
- 5Emirate health-information-exchange awareness. Some emirate exchanges expect visitor-to-patient joins to be policy-tagged at source. Test: ask for the exchange-policy field on the visitor record and the export job that respects it.
- 6Multi-site federation with central reporting. Most UAE hospital groups run four to twelve sites across two or more emirates; per-hospital SaaS cannot consolidate KPIs. Test: ask for the multi-site dashboard and visitor-volume report by ward and shift.
- 7Workflows for the six healthcare visitor classes. Each class needs different fields: contractor HSE induction, medical-rep consultant slot, trial-participant consent, auditor escort, medical-tourism group registration. Test: walk through all six.
- 8Infection-control screening at intake. UAE hospitals still maintain a declaration form, a thermal-screening flag and a visiting-hours gate for immunocompromised wards. Test: ask for the configurable declaration per ward and the refused-entry audit log.
- 9WCAG 2.2 AA accessible kiosk flow. A visitor with mobility or visual impairment must self-register at the self-service kiosk. Test: demonstrate a screen-reader run of the self-register flow.
- 10Badge printing with enterprise hardware partners. A £200 thermal printer that runs out of ribbon on Friday is unworkable; the VMS must drive Zebra, Honeywell or Epson hardware in a calibrated bilingual layout. Test: live print of a badge with photo, ward code and bilingual name.
- 11On-premises AI capability for visitor flow. On-prem AI for badge OCR, visitor-sentiment classification and intent triage is realistic for any hospital with a modest GPU. Test: ask which open-weight models they ship and whether inference runs inside the perimeter.
- 12WebRTC carer-room and remote-handover capability. Medical-tourism families and critical-care patients benefit from a WebRTC bridge without a public-cloud video service. Test: ask whether the VMS integrates with carer-room booking and the clinical telemedicine bridge.
- 13Fixed-fee phased engagement with weekly demos. CFO needs predictability; CIO needs steering control. Test: ask for a sample Discovery SOW and the demo cadence calendar.
- 1490-day exit window with full operator ownership at handover. The hospital must hold the repo, licence keys, deploy pipeline and runbook at handover. Test: ask what they hand over on day 91.
How do you choose between on-premises, sovereign cloud, and public-cloud SaaS in UAE hospitals?
For any UAE hospital handling PHI alongside visitor data, the answer in 2026 is sovereign on-premises by default.
| Dimension | Public-cloud SaaS | Sovereign cloud in UAE | Sovereign on-premises |
|---|---|---|---|
| Federal PDPL controller-processor posture | Vendor is processor, residency depends on clauses | Operator-aligned, residency in UAE | Operator is processor, data never leaves perimeter |
| Emirate health-exchange policy alignment | Indirect — relies on attestations | Direct — residency aligned to emirate | Direct — visitor table lives in the same datacentre as the clinical stack |
| Integration latency to the clinical stack | Public-internet round-trips for HL7/FHIR | LAN-adjacent if same regional DC | Sub-millisecond LAN integration |
| Operational continuity during connectivity loss | Check-in offline | Check-in offline | Continues on local stack |
| Per-visitor pricing pressure as the group grows | High — scales with volume | Medium | Zero — fixed-fee build |
| Source ownership at exit | None | Limited | Full handover, exit window honoured |
The pattern across UAE hospital groups is consistent: the federal PDPL DPO rules out public-cloud SaaS in the first compliance workshop, the emirate-exchange integration rules out anything that adds an internet round-trip, and the commercial discussion rules in the on-premises model.
> Want a fixed-fee Discovery price before the end of the call? Talk to Zeour engineering — 30-minute scoping conversation, no slideware, and a published pricing band by the time we hang up.
How much does visitor management cost in UAE hospitals in 2026?
- Discovery (3-6 weeks). £15k-£40k fixed-fee. Outputs: scored requirements register, integration map, federal PDPL impact-assessment input, bilingual badge mock, build SOW with milestone-fixed price.
- Build — single hospital (200-400 beds). £100k-£300k milestone-fixed. Reception + kiosk software, badge printing, HL7 v2 plus FHIR R4 integration, federal PDPL workflow, bilingual EN+AR full-RTL UI, infection-control declaration per ward, multi-class workflows, accessible kiosk.
- Build — multi-site UAE group (4-12 hospitals). £400k-£1.4M milestone-fixed. Adds multi-site federation, central reporting, group medical-office dashboard, emirate-exchange policy tagging, multi-emirate licensing rollups.
- Per-hospital hardware. £20k-£60k. Reception printers, kiosks, badge stock, ID-scanning hardware, access-control adapters.
- On-premises AI for visitor flow. £30k-£90k. GPU sizing, model selection, hardening, badge OCR pipeline, sentiment classifier.
- Care Plan. Tiered. From £40k-£180k annually.
The number not on this list is the per-visitor licence fee. Sovereign on-premises converts that into a fixed-fee build, after which the hospital owns the system. If a vendor's primary commercial mechanism is a per-visitor SaaS line that grows with each new site, model the seven-year total — on-premises is almost always cheaper inside three to four years.
ROI calculator — build a defensible business case in 7 steps
Step 1 — Baseline reception headcount and handle time
Count reception desks, FTE per shift, and average handle time. A 400-bed hospital with five reception points and 1,000 visitors per day at 3 minutes handle time consumes 50 reception-hours per day.
Step 2 — Project new handle time with kiosks plus VMS
A bilingual kiosk paired with a VMS reduces handle time to 60-90 seconds for self-service and 90-150 seconds for assisted visitors. A typical mix lands at 35 reception-hours per day.
Step 3 — Convert reclaimed time into capacity
The 15 reclaimed hours per day absorb medical-tourism registration peaks, infection-control declaration enforcement, and consultant-slot triage without adding headcount. Model 60 percent reabsorbed and 40 percent dropped to efficiency.
Step 4 — Quantify clinical-safety risk reduction
The avoided cost of a single infection-control breach traceable to a misclassified visitor entering an immunocompromised ward sits in the high five to low six-figure range. Ward-level enforcement reduces probability materially.
Step 5 — Quantify the medical-tourism revenue lift
Medical-tourism patients with carer and family are price-sensitive on experience — a digital front door from pre-arrival appointment through wayfinding to feedback is the differentiator. A 1 percent uplift in inbound case mix at a 200-bed hospital is typically a six- to low seven-figure annual revenue swing.
Step 6 — Subtract seven-year total cost of ownership
Add Discovery plus Build plus hardware plus optional on-premises AI plus seven years of Care Plan plus internal change cost. Divide by seven.
Step 7 — Compare against the seven-year SaaS counterfactual
Project the per-visitor SaaS line at projected daily volume, scaled for group growth. In every UAE multi-site group we have modelled, on-premises is cheaper by year three.
Seven failure modes from UAE hospital VMS deployments
Failure 1 — public-cloud SaaS chosen before the PDPL workshop. Signs in Q1, runs the PDPL impact assessment in Q3, finds residency does not meet the DPO brief, tears out in Q4. Run the PDPL workshop first and longlist only sovereign on-premises vendors.
Failure 2 — bilingual EN+AR retrofitted, not engineered. The vendor demonstrates English-only, promises Arabic in v4.2, ships a string-table translation that breaks bidirectional layout, the matron files a clinical-safety incident. Full-RTL must be at the framework layer; demand the badge-print proof in Discovery.
Failure 3 — no integration to the clinic stack. The VMS asks the receptionist to type the visited patient's name and maintains its own patient table, which drifts out of sync with admissions. Fix: HL7 v2 plus FHIR R4 on day one — the electronic medical record and visitor table must share host-patient identity.
Failure 4 — single-tenant per-hospital deployment in a group. The group medical office cannot consolidate KPIs, central security cannot push a policy change, IT runs four to twelve separate upgrade cycles. Use multi-site federation from day one.
Failure 5 — visitor-class workflows collapsed into one flow. Contractors, medical reps, trial participants and medical-tourism families are forced through the same six-field form, which loses the medical-tourism family entirely. Run six distinct workflows — see the enterprise visitor check-in workflow playbook.
Failure 6 — accessible kiosk flow ignored. The kiosk ships with accessibility off, a visitor in a wheelchair cannot reach the screen, the JCI surveyor flags it. Bake WCAG 2.2 AA into the kiosk specification at procurement.
Failure 7 — vendor lock-in at exit. At year four the visitor history is in a proprietary schema with no export, the portal is on the vendor's domain, the licence is non-transferable. Embed the 90-day exit window from day one.
Migration path
Phase A — stabilise the legacy. Lock the paper or SaaS system, freeze configuration changes, extract a clean visitor-history export, complete the federal PDPL impact assessment. Two to four weeks.
Phase B — pilot one hospital. Deploy the sovereign on-premises stack at the flagship 300-500-bed site. Wire HL7 v2 plus FHIR R4 to the clinic stack. Train reception, security, infection control and the matron's office. Parallel run two weeks, cut over. Eight to twelve weeks.
Phase C — roll out across the group. Replicate at one site every two to four weeks. Each site inherits central configuration, applies per-site overrides for ward count and visiting-hours policy, joins central reporting from go-live. Twelve to twenty-four weeks for a four-to-eight-site group.
Phase D — operate and improve. Care Plan kicks in, on-premises AI is enabled for badge OCR and sentiment if scoped, the group medical office publishes the first consolidated dashboard, and the next-year roadmap covers WebRTC carer-room expansion and feedback via the customer feedback system. Continuous.
Implementation playbook
The five-stage cadence below is what we have run across the UAE healthcare sector and the wider GCC, including the production reference at the Ministry of Health Kuwait — a GCC healthcare deployment whose architectural patterns translate cleanly to the UAE hospital context.
- 1Discovery (3-6 weeks, fixed-fee £15k-£40k). Workshops with reception, security, infection control, IT, DPO, clinic-stack lead, medical office and procurement. Outputs: scored requirements register, integration map, bilingual UI mock, badge-print proof, federal PDPL inputs, build SOW.
- 2Build (12-28 weeks, milestone-fixed). Reception software, kiosk software, badge printing, multi-class workflows, bilingual EN+AR full-RTL UI, infection-control declarations per ward, central administration portal, multi-site federation harness. Weekly demos Fridays; steering Tuesdays.
- 3Integrate (last 8-12 weeks of Build). HL7 v2 plus FHIR R4 to the clinic stack, the online appointment system for pre-arrival, the queue management system for post-reception, the wayfinding system for navigation, the digital signage system for reception screens, emirate-exchange policy tagging on the visitor record.
- 4Pilot plus Go-Live (4-8 weeks per site). Pilot one site, parallel run two weeks, cut over, roll out across the group.
- 5Operate (continuous). Care Plan with response-time SLAs, on-premises AI roll-in if scoped, weekly KPI publishing, quarterly steering, annual federal PDPL refresh.
Frequently asked questions
How does a UAE hospital VMS comply with the federal Personal Data Protection Law?
The federal PDPL treats the visitor record as personal data and, when linked to ward and time, as health-adjacent data warranting elevated protection. The VMS must capture lawful basis, expose data-subject-rights workflows, enforce retention and deletion, and keep the record inside the hospital perimeter. A sovereign on-premises deployment satisfies all four in one decision.
Does the VMS need to integrate with the emirate-level health information exchange?
Yes — emirate-exchange policies expect visitor-related data linked to a patient to carry policy markers when exchanged. The VMS must support the policy field on the visitor record and respect it on export. The integration is operator-direct rather than vendor-mediated, which is another argument for the on-premises architecture.
How do we handle medical-tourism visitors arriving with carer and family?
A dedicated workflow registers the group as a unit, allocates the patient to a clinical pathway and the carer plus family to a hospitality pathway, prints role-specific bilingual badges, books the carer into a WebRTC family room when clinically appropriate, and feeds the post-discharge experience into the feedback system. See the hospital outpatient digital front door playbook.
Can the VMS share infrastructure with the clinic management system?
Yes — and it should. The visitor and patient tables share enough identity context that disjoint infrastructure adds latency and integration risk. One operator-owned on-premises stack with clinic management, EMR and VMS sharing storage and identity is the reference architecture. See the bilingual on-premises clinic management buyer's guide.
How does the VMS support JCI accreditation cycles?
The VMS provides the audit trail JCI surveyors expect for the patient and visitor rights chapter, the infection-control declaration log, the permit-to-work record, and accessible-kiosk evidence under WCAG 2.2 AA. The matron's office pulls these from the central dashboard without IT involvement.
What does the bilingual EN+AR experience look like at the kiosk?
The visitor selects language at the welcome screen, every subsequent screen renders with proper bidirectional layout, the badge prints with both scripts in a calibrated layout that does not clip Arabic ligatures, and SMS confirmations land in the chosen language. The product reference is the bilingual baseline capability shipped across the Zeour stack.
How does on-premises AI improve the visitor experience without sending data to a cloud LLM?
Open-weight models on the hospital's own GPUs perform badge OCR (without sending the image off-site), sentiment classification on post-visit feedback (without sending PHI to a public LLM), and intent triage of the reception walk-up queue. Same pattern as the AI clinical assistant inside MediCare deployments.
How does the VMS interact with queue management at the reception?
The VMS registers the visitor and creates a queue ticket for the next flow — pharmacy, billing, escort to ward, or carer-room induction. The same identity threads through both systems. The UAE queue management healthcare guide covers the queue side.
What happens if internet connectivity drops?
The sovereign on-premises model continues operating on the hospital LAN. Reception keeps printing badges, kiosks keep registering visitors, and central reporting catches up once connectivity returns. A public-cloud SaaS stops at the front door — which is why every UAE hospital that has lost internet during a sandstorm or fibre cut revisits the architecture at the next procurement cycle.
How do we handle compassionate visits outside scheduled hours?
Visiting-hours policy is configurable per ward and shift, with an override flow authorised by a duty manager. The override is logged with manager identity, reason code, and timestamp, which satisfies the JCI surveyor and infection-control lead. The visitor receives a time-limited badge with the override indicator visible to ward staff.
Where Zeour fits
Zeour Ltd is a UK-registered company shipping a sovereign on-premises, bilingual EN+AR, fixed-fee enterprise stack — visitor management, clinic management, queue management, online appointment, self-service kiosk, wayfinding and customer feedback — to operators worldwide, with regional strength across the GCC and MENA. The production portfolio spans 1,247+ branches across 40+ countries; the GCC reference at the Ministry of Health Kuwait demonstrates the pattern at ministry scale. UAE hospital engagements follow the same posture: sovereign on-premises by default, bilingual full-RTL at the framework layer, integrated on HL7 v2 plus FHIR R4 plus DICOM and WebRTC, fixed-fee phased with a 90-day exit window, on-premises AI on operator hardware. The horizontal compliance buyer's guide covers GDPR, HIPAA and PDPL together, the KSA government VMS guide addresses the public-sector cousin, the healthcare industries hub maps the wider vertical, and a fixed-fee Discovery price is one contact form away.
--- Last updated: May 18, 2026 — by the Zeour engineering team.