Key takeaways
- Oman healthcare buyers are converging on a clear pattern. Modern outpatient flow demands on-premises patient data, a bilingual Arabic-English baseline with full RTL, integration with national e-health via standard interoperability, and AI that stays inside the hospital perimeter. Cloud-only generic platforms cannot meet this brief.
- PDPL changes how you specify a queue management platform. The Oman Personal Data Protection Law (Sultani Decree 6/2022) treats clinical encounter data as sensitive personal data, elevating sovereign deployment, audit-grade logging, and DSAR workflows into procurement-spec requirements.
- Bilingual is a framework decision, not a translation pass. Patients expect Arabic-first interfaces; clinicians expect English-first dashboards. The system must switch the entire UX — kiosks, ticket stubs, SMS — in one operation. See bilingual baseline.
- Outpatient flow is multi-stage. A visit passes through registration, triage, consult, imaging, lab, pharmacy, cashier, follow-up. Each stage needs queue intelligence that knows about the others. The clinic management system pattern handles this as a workflow.
- Costs in Oman sit in defined ranges. Discovery £15k-£40k; small Build £80k-£220k; enterprise Build £300k-£900k. Per-clinic hardware £6k-£18k.
- Procurement is shifting toward fixed-fee phased engagements with operator self-sufficiency at exit. A 90-day exit window is the contractual pattern that protects budget and capability.
- On-premises AI is now standard. Oman hospital IT leads increasingly ask for an AI clinical assistant on the hospital's own GPU — no PHI leaving the perimeter.
This guide is for healthcare buyers in Oman scoping a queue, appointment, and outpatient flow programme for 2026. It is opinionated about the regulatory context — Ministry of Health, Vision 2040 Strategic Pillar of Human Development, Oman PDPL, TRA cybersecurity guidance — and equally opinionated about the engineering posture that delivers durable value across healthcare.
Who this guide is for
Four personas should read this end-to-end.
The Ministry of Health IT director. You own the digital backbone of public outpatient capacity across Oman's governorates. Stakeholders include MoH leadership, the national e-health team, and the TRA on cybersecurity. You need a platform that talks cleanly to clinical records via HL7 v2 and FHIR R4 endpoints, supports a fully bilingual patient interface, and procures under fixed-fee terms.
The multi-site private hospital group CIO. You operate three to twelve hospitals across the Muscat capital area, the Batinah coast, Dhofar, and inland governorates. KPIs are throughput, patient experience, and cost-per-encounter. You need a platform governed centrally but executed per-site, with local fall-back so a regional outage does not stop the queue at Sohar.
The primary-care centres director. You run 8 to 30 polyclinics or family-medicine centres. Volume is dominated by chronic follow-up, paediatric immunisation, antenatal care, and acute walk-in. The platform has to make routine appointments self-service while preserving walk-in capacity, bilingually, with minimal staff training.
The patient experience director. You sit between operations, clinical leadership, and brand. You are measured on satisfaction, complaint volume, and digital adoption. You need quantified evidence that the platform reduces perceived wait time and feeds into service-design through a structured customer feedback system.
What is healthcare queue management in 2026 — and why it's different for Oman?
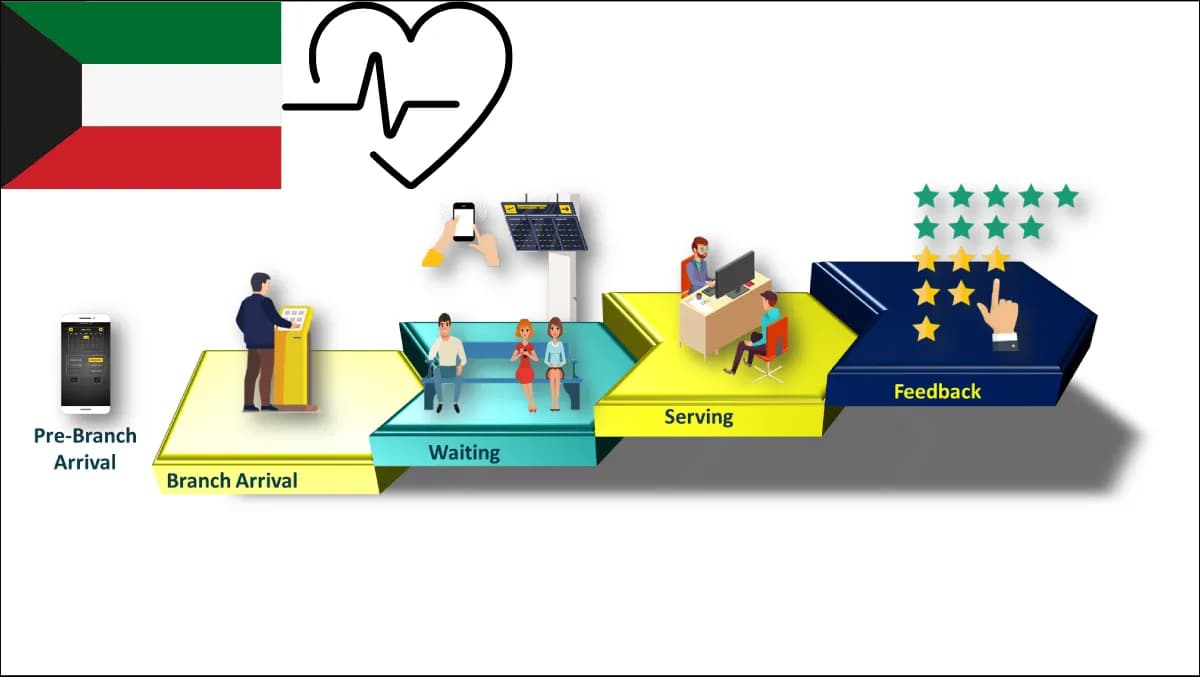
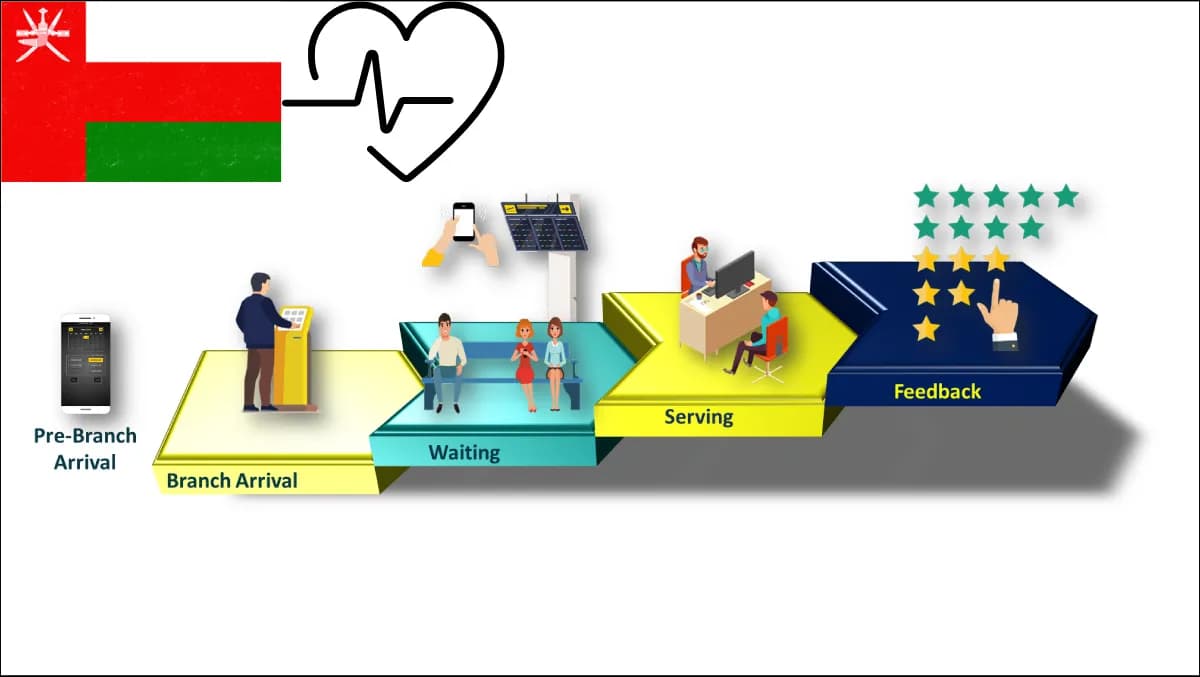
In 2026, healthcare queue management has stopped being a ticket-dispenser-plus-display product and has become a clinical-flow orchestration platform. The unit of value is no longer a ticket — it is the patient journey across registration, triage, consultation, diagnostics, dispensing, payment, and follow-up. Every interface the patient touches must know where they are and what comes next.
Three shifts make Oman different from a generic Gulf brief.
The first is Vision 2040, specifically the Strategic Pillar of Human Development, which sets healthcare quality, access, and digital-service maturity as central outcomes. Buyers must demonstrate measurable improvements in patient experience and bilingual accessibility, not just operational uptime. A platform that cannot produce that evidence will not pass the next budget cycle.
The second is Oman PDPL — Personal Data Protection Law under Sultani Decree 6/2022 — administered alongside MTCIT guidance and TRA cybersecurity expectations. Clinical encounter data and queue-state telemetry that links a national ID to a clinic visit fall under sensitive personal data. Operators must apply lawful-basis discipline, data-minimisation, and demonstrable data-subject access. The data-handling story has to be defensible to the regulator.
The third is the national e-health platform pattern. The Ministry of Health is operating a national health-information environment connecting primary, secondary, and specialist care through standard interoperability. Your queue platform must integrate cleanly without becoming a parallel record system — HL7 v2 feeds for ADT and orders, FHIR R4 endpoints for demographics and appointments, DICOM awareness for imaging, with a clear contract on which system owns which fact.
On top of those, the bilingual baseline is non-negotiable. Patients expect Arabic-primary UX; clinicians expect English-first dashboards with Arabic available for shared documentation. Zeour ships every product with English and Arabic full RTL as the production baseline.
For regional context see our parallel guides on Saudi healthcare, UAE healthcare, and Kuwait healthcare. Each market differs in regulator wording; the engineering posture rhymes.
The Oman-fit scoring rubric — 14 criteria
Score any vendor proposal 0-3 per criterion (0 = absent, 3 = excellent). A credible Oman healthcare deployment should clear 32 out of 42.
| # | Criterion | What good looks like |
|---|---|---|
| 1 | PDPL alignment | Documented lawful basis, data-minimisation, DSAR workflow, breach-notification runbook. |
| 2 | On-prem or in-country option | Full deployment behind the hospital firewall on the operator's hardware. |
| 3 | EN + AR bilingual baseline | Whole UX — kiosks, mobile, displays, SMS, printable tickets — switches in one operation. |
| 4 | HL7 v2 ADT integration | Real-time admit-discharge-transfer feeds from the clinical record system. |
| 5 | FHIR R4 endpoints | Patient, Appointment, Encounter, Practitioner resources exposed and consumed. |
| 6 | DICOM awareness | Queue platform understands imaging order state, not just generic queue stage. |
| 7 | National e-health platform interop | Clear contract for which system owns which fact, no duplicate records. |
| 8 | Bandwidth resilience | Branch-level local fall-back; regional outages do not stop ticket-calling. |
| 9 | Outpatient multi-stage workflow | Registration to triage to consult to imaging to lab to pharmacy to cashier as one journey. |
| 10 | Walk-in vs appointment balance | Configurable per clinic, by hour, by clinician availability. |
| 11 | Bilingual SMS notification stack | Local SMS aggregator integration with Arabic + English templates. |
| 12 | Accessibility | WCAG 2.2 AA for kiosks and patient mobile interface. |
| 13 | Fixed-fee phased delivery | Discovery fixed, Build milestone-fixed, exit window contractual. |
| 14 | Operator self-sufficiency | Code, configuration, runbooks, training delivered such that operator runs without vendor. |
For cross-discipline context, see the hospital outpatient digital front door playbook and the clinic management system bilingual on-prem buyer's guide.
How do you choose between on-premises, sovereign cloud, and public-cloud SaaS in Oman?
PDPL plus TRA cybersecurity guidance plus multi-governorate bandwidth realities push the answer toward on-premises by default for PHI.
On-premises means application and database run on hardware inside the hospital perimeter. PHI, queue-state telemetry, and AI inference all stay on hospital infrastructure. PDPL DSARs are answered from your own systems, with no third-party processor in the chain. Default Zeour posture for Oman healthcare.
Sovereign cloud — a private-tenant cloud hosted physically inside Oman — is a defensible middle ground for non-PHI: marketing site, analytics dashboards, configuration consoles. Not the right posture for live patient queue state if your PDPL impact assessment classifies it as protected.
Public-cloud SaaS is the easiest to procure and the worst long-run fit for an Oman programme handling protected data. Data on a hyperscaler tenant in a foreign jurisdiction is a regulator concern; every queue interaction depending on internet uptime to a foreign data centre is a clinical concern.
The practical Oman pattern: deploy on-premises at every hospital and large polyclinic; let the central CIO console ride on a sovereign-cloud tenant inside Oman if operationally useful; never put PHI on a public-cloud SaaS surface.
> Call-out — the PDPL lens. If your procurement spec does not ask "where is PHI stored, processed, and analysed at every moment in the patient journey?" your spec is incomplete. The answer should be defensible to the regulator on a Tuesday morning without legal counsel in the room.
How much does healthcare queue management cost in Oman in 2026?
Bands below are drawn from Zeour engagements in Oman and the surrounding Gulf, quoted in pounds sterling; local-currency conversion happens at Discovery.
| Programme shape | Indicative range | What's included |
|---|---|---|
| Discovery | £15k-£40k | Per-site flow audit, integration spike, fixed-fee SOW for Build. |
| Build (small) | £80k-£220k | Single hospital or 4-10 polyclinic network; full GLARUS stack; bilingual; basic integrations. |
| Build (enterprise) | £300k-£900k | Multi-hospital private group or Ministry network; deeper integrations; AI pilot. |
| Integrations | £20k-£70k per external system | Per-system effort for EMR, lab, imaging, pharmacy, payment, national e-health endpoint. |
| Per-clinic hardware | £6k-£18k | Self-service kiosks, calling displays, ticket printers, signage, network gear. |
| Care Plan | £40k-£180k annually | Uptime monitoring, regulatory-change updates, minor enhancements. |
Ranges are wide because scopes vary: a specialty clinic in Muscat is not the same procurement as a Ministry network serving Dhofar, Al Batinah, and the interior. What ranges share is posture — every line is fixed-fee or milestone-fixed. See also our pricing page.
ROI calculator — build a defensible business case in 7 steps
The board cares about throughput, patient experience, complaint volume, and cost per encounter. Seven steps translate the investment into a case any Oman healthcare board will sign.
Step 1 — Baseline current outpatient flow. Three months of data: encounters per clinic per day, reception wait, triage-to-consult wait, total visit duration, no-show rate, walk-in-to-appointment ratio. If you cannot answer these, that gap is itself a finding.
Step 2 — Quantify wasted patient-time hours. If 800 patients each lose 22 minutes to avoidable wait, that is 293 patient-hours per day per hospital. Multiply by network size.
Step 3 — Quantify clinician-time lost to flow friction. Clinicians who spend 18 minutes per session waiting for the next patient represent direct capacity loss at the most expensive labour rate in the building.
Step 4 — Estimate no-show reduction. Bilingual SMS plus mobile confirmation reduces no-show rates by 20-40% across Gulf programmes. Translate into recovered appointment capacity.
Step 5 — Estimate the bilingual-accessibility lift. Arabic self-service reduces reception load — freed FTE redeployable to walk-in handling.
Step 6 — Compare against three-year TCO. Build plus three Care Plans plus hardware refresh. Small Build over three years lands £200k-£500k; enterprise £600k-£1.6M. Compare against recovered hours from steps 2-5.
Step 7 — Add the regulator-trust line. A board operating within PDPL, with on-prem PHI and audit-grade logging, does not put quarterly time into regulator briefings.
Seven failure modes from Oman deployments
Failure mode 1 — bilingual as a translation file. Vendors hand the operator a spreadsheet to translate; the result is broken RTL, mismatched fonts, overflowing ticket stubs, SMS templates that send English to Arabic-preferring patients. Fix: framework-bilingual end to end.
Failure mode 2 — queue platform that does not understand outpatient stages. Generic ticketing calls patients to a counter; outpatient flow requires a workflow that knows about triage, consult, imaging, lab, pharmacy, and cashier as distinct stages with different SLAs. See the online appointment system reference pattern.
Failure mode 3 — no resilience for regional connectivity. A cloud-only deployment fails at the polyclinic in a remote governorate the moment the internet hiccups. Patients sit; staff revert to paper; credibility collapses. Fix: branch-level local execution with central rollups.
Failure mode 4 — PHI leaking to vendor SaaS. A cloud-only vendor stores patient names, national identifier numbers, and visit-reason text on a foreign hyperscaler tenant. PDPL impact assessment becomes impossible to defend. Fix: on-prem PHI, period.
Failure mode 5 — no operator self-sufficiency at exit. Vendor disappears into a recurring SaaS bill; operator cannot make cosmetic changes without a paid ticket. Three years later the renewal is unaffordable and migration cost equals the original Build. Fix: contractual exit window and operator-runnable runbooks at handover.
Failure mode 6 — AI assistant that calls an external API. A clinical-decision feature that POSTs patient summaries to a foreign API turns every clinical note into a PDPL incident. Fix: AI on the hospital's own GPU server.
Failure mode 7 — no feedback loop. A queue platform that does not feed into a structured patient-experience programme is a dashboard the board never opens. Fix: pair the queue with a real customer-feedback surface and route findings into a quarterly service-design review.
Migration path — replacing a legacy queue platform without a clinical incident
Most Oman hospital groups have some queue system already. Replacing it without disrupting clinical operations follows a specific pattern.
Stage 1 — site survey, two weeks. Walk every site. Document the actual flow, not the documented one. Map every integration touchpoint with the electronic medical record, lab, pharmacy, cashier, and national e-health platform. Identify bilingual-content gaps.
Stage 2 — pilot site selection, one week. One large (complexity), one small (rollout rehearsal). Avoid flagship-only — patterns that work at the flagship rarely scale unchanged.
Stage 3 — build and integration, eight to twelve weeks. Milestone-fixed sprints with weekly demos. HL7 v2 ADT and FHIR R4 integration dominates. Bilingual review runs in parallel.
Stage 4 — pilot, four to six weeks. Both sites live, legacy retained as fall-back. Measurements: wait-time distribution, complaint volume, staff feedback, integration error rate.
Stage 5 — rollout, three to nine months. Wave-based, three to six sites per wave, operator-shadowed. Legacy decommissioned site by site.
Stage 6 — Care Plan, ongoing. Twelve-month default covering uptime monitoring, regulatory updates, minor enhancements.
Implementation playbook — what a Zeour Oman healthcare engagement looks like
Four phases.
Discovery — fixed fee, four to eight weeks. Senior engineer on-site. Per-site flow audit. Integration spike against clinical record, lab, imaging, pharmacy, cashier, and national e-health endpoint. Bilingual review. PDPL alignment with operator's legal team. Output: fixed-fee SOW for Build.
Build — milestone-fixed, twelve to thirty-two weeks. Queue management at every site. Online appointment for self-service with bilingual UX. Virtual queueing for mobile remote-join. Wayfinding for multi-floor hospitals. Customer feedback for post-visit capture. MediCare clinic management where the operator runs Zeour's clinical workspace. AI clinical assistant pilot on-premises with optional WebRTC telemedicine.
Pilot — four to six weeks. Two pilot sites live. Weekly governance with clinical, IT, and CX leadership; daily standup with operator team. The point is to rehearse the rollout pattern, not just to validate software.
Rollout — three to nine months. Wave-based, partner-led, operator-shadowed. Zeour's job becomes coaching by month four. Operator self-sufficiency is the contractual measure.
Care Plan — ongoing. Twelve-month default. Operator owns code, configuration, runbooks, and decision authority. The 90-day exit notice is the operator's asset.
For Oman cross-reference see our OQBI Oman case study — banking, same fixed-fee on-prem posture. For the closest Gulf healthcare reference see the MoH Kuwait case study.
Frequently asked questions
Does the Oman Personal Data Protection Law require us to keep patient queue data on-premises?
The law does not require a specific topology; it requires that processing of sensitive personal data meets lawful-basis, data-minimisation, security, and data-subject-rights standards. Defending those standards is materially easier when PHI remains on-prem inside the hospital perimeter. Our recommendation: on-prem for PHI by default, non-PHI components on in-country sovereign cloud where operationally useful. See the PDPL glossary entry.
How does the platform integrate with the national e-health platform?
Via standard healthcare interoperability — HL7 v2 messaging for ADT and orders, FHIR R4 endpoints for patient, appointment, encounter, and practitioner resources. The contract is explicit about which system owns which fact: the national platform owns the longitudinal record, the hospital's clinical record system owns the encounter, the queue platform owns the in-visit workflow state. No duplicate record-keeping, no shadow patient store.
Does the system work in both Arabic and English?
Yes — and the bilingual capability is framework-deep, not a translation overlay. The entire patient-facing experience including kiosks, mobile join, calling displays, printed tickets, and SMS notifications switches between Arabic and English in one operation. Clinicians use English-first dashboards with Arabic available where shared clinical documentation requires it. The Zeour bilingual baseline is production-grade across the portfolio.
Can the platform handle multi-stage outpatient workflows — triage, consult, imaging, lab, pharmacy, cashier?
Yes. The platform models the patient journey as one workflow with stages that know about each other. A patient who completes consultation with an imaging order automatically appears in the imaging queue with priority informed by triage class and dwell time. The cashier sees the patient when consult and diagnostics complete; the pharmacy receives the e-prescribing trigger from consult. This is the headline difference between a generic queue product and a workflow platform like the MediCare clinic management system.
What integrations are most common in Oman hospital deployments?
The common set: clinical record system via HL7 v2 ADT and FHIR R4; lab system; imaging via DICOM work-list awareness; pharmacy for prescribing handoff; cashier for billing-state synchronisation; national e-health endpoint per the agreed contract; SMS aggregator for bilingual notification; local single-sign-on directory for clinician auth. Most engagements run four to eight active integrations.
How do you support polyclinics in remote Oman governorates with intermittent connectivity?
Branch-level execution. Every site runs a local instance fully functional during a network event — patients are checked in, tickets called, workflow proceeds. When connectivity returns, the local instance reconciles with the central rollup. Patients in Dhofar or the interior never see a connectivity-driven service interruption.
Can we run an AI clinical assistant without sending patient data to a foreign cloud?
Yes — this is the most-asked question from Oman hospital IT directors in 2026. The Zeour pattern runs the AI assistant on the hospital's own GPU server, using open-weight large language models, with retrieval against the hospital's own knowledge base. No PHI leaves the perimeter. See on-premises AI.
What does the Care Plan cover and what is the 90-day exit window?
Care Plan is the post-Build operate phase: uptime monitoring, regulatory-change updates (PDPL evolution, MoH guidance, national e-health endpoint changes), minor enhancements, incident response — fixed annual fee. The 90-day exit window is the operator's contractual right to terminate Care Plan on 90 days' notice, at which point Zeour delivers code, configuration, runbooks, and final training so the operator runs in-house. The point is not that it gets exercised — it is that it changes the negotiation balance permanently.
How long does a typical Oman healthcare programme take from contract to go-live?
Small Build (single hospital or 4-10 polyclinic network): Discovery four to six weeks, Build twelve to eighteen weeks, Pilot four weeks, Rollout three to four months. Total: roughly six to nine months. Enterprise Builds extend to nine to fifteen months depending on integration depth. We commit to these timelines in the Statement of Work.
How do we run a meaningful pilot without disrupting patient care?
Clinical leadership picks two sites where pilot risk is acceptable. Legacy stays live as fall-back. Pilot starts with one clinic per site, expands to full site over two weeks, runs four weeks at full scale. Daily standup with reception leadership surfaces issues within hours; weekly governance tracks pilot KPIs. Legacy is decommissioned only when KPIs are met.
Where Zeour fits
Zeour Ltd is a UK-registered company shipping a 12-solution enterprise platform worldwide, with regional strength in the Gulf and MENA. We have shipped queue and customer-flow programmes across the GLARUS ecosystem to 1,247+ branches in 40+ countries, including production deployments in Oman across regulated sectors.
Six things consistently matter to Oman healthcare buyers in 2026.
First, sovereign on-premises by default. PHI, queue-state telemetry, and AI inference stay inside the hospital perimeter. PDPL-defensible by design.
Second, engineered multilingual — Arabic and English full RTL as the production baseline across every product, other locales addable per engagement. No translation-overlay shortcuts.
Third, production portfolio as proof. Every product is real and deployed. References available under NDA.
Fourth, fixed-fee phased engagements. Discovery fixed-fee; Build milestone-fixed with weekly demos; 90-day exit window contractual; operator self-sufficiency at exit is the deliverable.
Fifth, on-premises AI without giving up capability. Open-weight LLMs on the operator's own GPU server with retrieval against the operator's knowledge base.
Sixth, worldwide reach with regional strength. We deliver from London across UK, EU, and Americas, and through a certified delivery network across the Gulf, MENA, Africa, and Asia.
If you are scoping a healthcare queue, appointment, or outpatient flow programme for 2026, talk to us via our contact page. Discovery is fixed-fee and delivers a defensible Statement of Work.
---
Published May 17, 2026 by Zeour Engineering. Zeour Ltd ships a 12-solution enterprise platform worldwide. Arabic and English full RTL ship as production baseline; any locale addable per engagement.