Key takeaways
Kuwait healthcare buyers in 2026 are not shopping for a generic ticket dispenser. They are buying a clinical-grade patient-flow platform that satisfies MoH Kuwait operational expectations, the Kuwait Data Privacy Protection Regulation issued by CITRA, and the Health pillar of Kuwait Vision 2035 — while remaining bilingual, sovereign, and interoperable with the wider clinic management stack.
- Patient health information has to stay inside Kuwait under the Kuwait Data Privacy Protection Regulation; sovereign on-premises deployment is the default posture.
- Bilingual EN+AR with full right-to-left is non-negotiable across tickets, kiosks, displays, SMS, and clinician consoles — proven at the framework layer, not as a translation overlay.
- Integration is almost always HL7 v2 for ADT and orders, FHIR R4 for modern endpoints, and DICOM for imaging.
- Outpatient flow in Kuwait is shaped by primary-care centres feeding hospital specialty clinics; your queue model must handle that referral pattern natively.
- The Health pillar of Kuwait Vision 2035 prioritises patient experience and digital citizen services; QMS sits inside that programme.
- 2026 cost bands: Discovery £15k-£40k, Build small £80k-£250k for a multi-site primary-care or single-hospital deployment, enterprise £300k-£1M for ministry-scale or large hospital group rollouts.
- The right delivery model is fixed-fee phased engagement with a 90-day exit window, weekly demos, an operator-owned repo at the end, and an on-premises AI Clinical Assistant option that runs on the operator's hardware.
This guide walks a Kuwait MoH IT director, a multi-clinic hospital group CIO, a primary-care centres director, and a patient-experience director through what to specify, how to score vendors, and how to phase the rollout.
Who this guide is for
Four personas drive most Kuwait healthcare QMS conversations in 2026.
Kuwait MoH IT director. You are responsible for primary-care centres and hospital outpatient flow across the country, integrating into the national health information pattern, and ensuring CITRA cybersecurity requirements are met. You care about a sovereign deployment topology that fits inside the ministry's existing data-centre footprint and survives an annual audit.
Multi-clinic hospital group CIO. You run a private group with two to eight sites across Kuwait City, Hawalli, Farwaniya, Ahmadi, and Jahra. You need one platform that gives head office consolidated reporting and lets each clinic configure local hours, services, and clinician panels. Bilingual baseline, on-prem PHI, and a tight integration with your clinic management system decide the deal.
Primary-care centres director. You manage walk-in flow across family-medicine centres and want to introduce virtual queueing, online appointments, and forecastable wait times. Your KPIs are average wait time, walk-away rate, and patient satisfaction.
Patient-experience director. You sit between clinical operations and marketing. You care about feedback capture at the right moment, wayfinding signage that reduces lost-patient anxiety, and a measurable NPS uplift you can defend in a board paper.
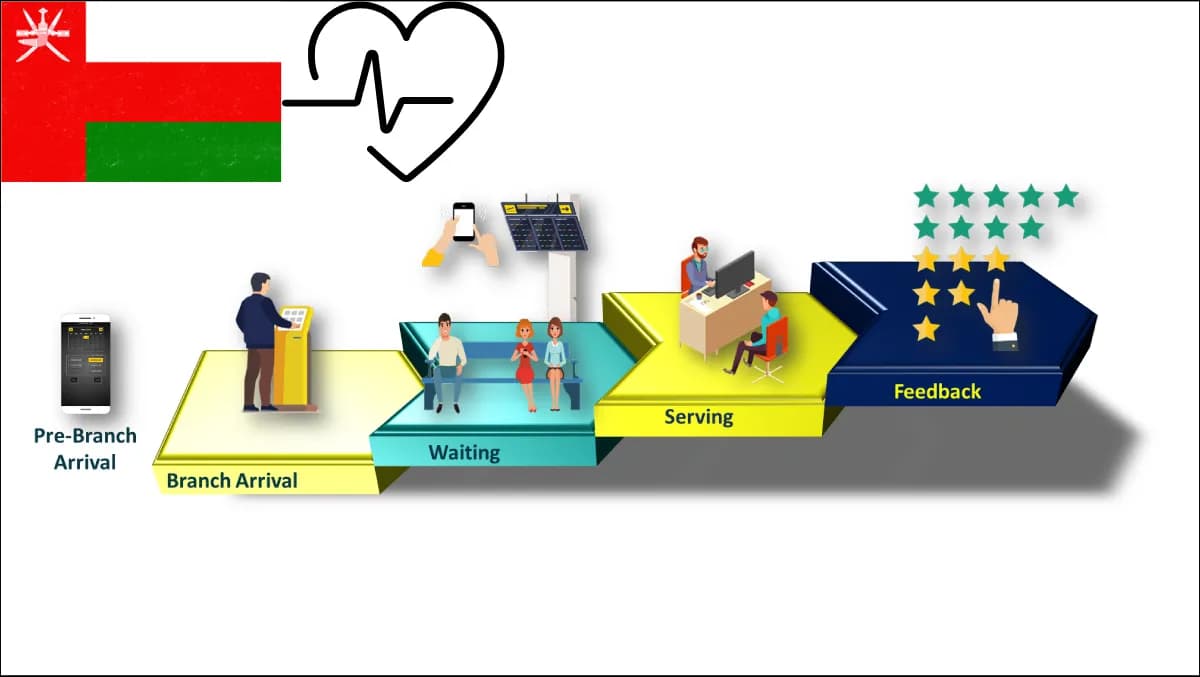
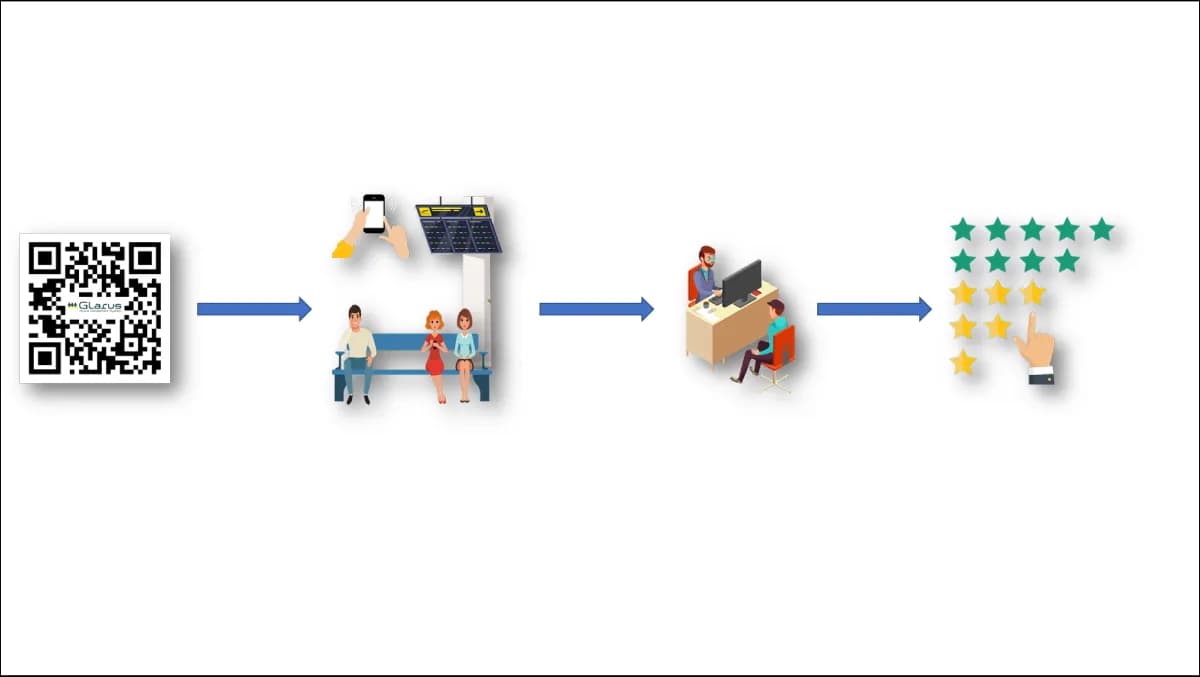
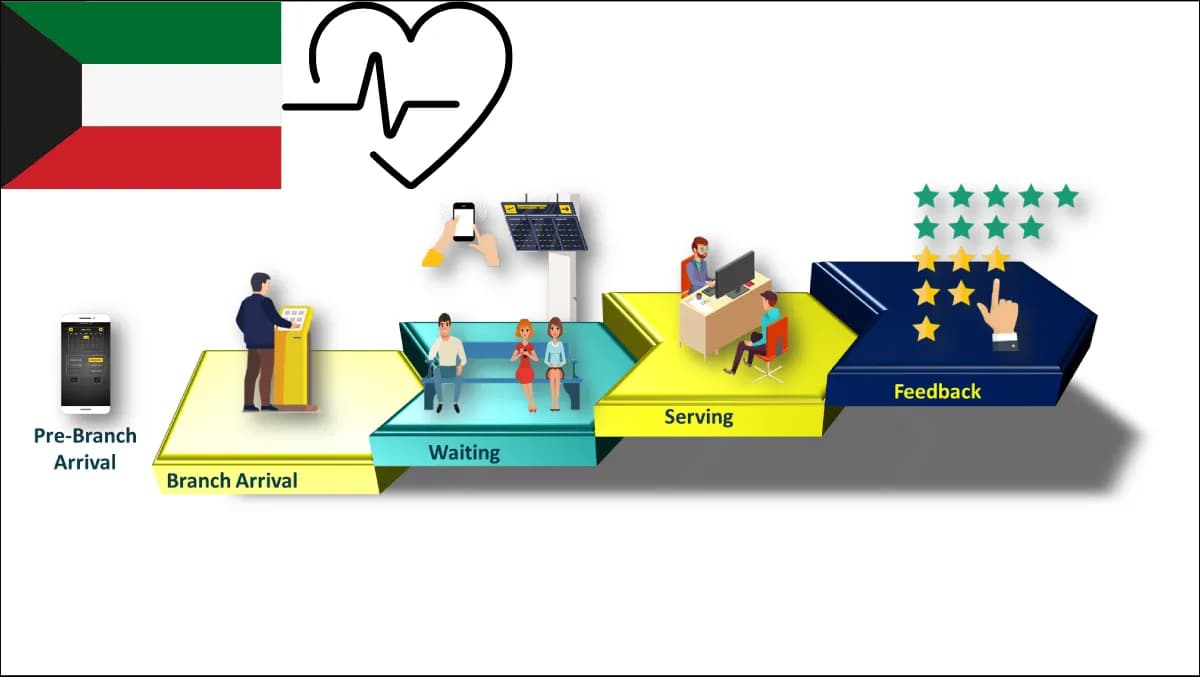
What is healthcare queue management in 2026 — and why it's different for Kuwait?
A modern healthcare queue management system is no longer a single-screen ticket dispenser. It is a patient-flow control plane spanning pre-arrival check-in via SMS or web, kiosk check-in with national identity verification, queue creation against a service that maps to a clinician panel, real-time call-forward consoles, bilingual signage, virtual queueing, real-time analytics, and integration into the hospital information system so appointments, tickets, and clinical encounters share one patient identifier.
Kuwait sharpens this profile in four ways.
First, the data law is sovereign. The Kuwait Data Privacy Protection Regulation issued by CITRA expects personal data — and patient health data in particular — to be processed under defined controls, with explicit consent, retention discipline, and breach-notification obligations. The simplest path to compliance is keeping PHI on infrastructure you operate, inside Kuwait. That maps directly to a sovereign on-prem topology, not a public-cloud SaaS subscription.
Second, bilingual Arabic and English is mandatory. Every patient-facing surface — ticket, kiosk, signage, SMS, web booking, clinician console — has to render perfectly in both directions. This is a framework-level concern, not a translation overlay. Zeour ships bilingual EN+AR as a production baseline, with full right-to-left layout, locale-aware numerals, currency, and dates, and PDF rendering that picks the correct script.
Third, integration is real. A Kuwait clinic or hospital almost always has an existing electronic medical record, a laboratory information system, a radiology information system with DICOM-attached modalities, and a pharmacy system. Your QMS has to speak HL7 v2 for ADT and orders, expose FHIR R4 endpoints, and respect the patient identifier the EMR considers authoritative.
Fourth, the national health information pattern matters. Kuwait operates a national health-data network that connects MoH-aligned providers, and your platform has to participate in that pattern where required without leaking PHI outside the perimeter. Confirm the operator's specific integration spec during Discovery rather than promising compatibility with a moving target.
The practical impact is that the right QMS for Kuwait healthcare looks much more like a clinical workflow platform than a ticket dispenser. See the healthcare industry page for the full positioning.
The Kuwait-fit scoring rubric — 14 criteria
Use this as a procurement scoring template. Score 0-5 per criterion and weight per your priority. A vendor that scores well across the rubric will survive a CITRA audit, a clinical-safety review, and a five-year change cycle.
| # | Criterion | What "5" looks like |
|---|---|---|
| 1 | Sovereign on-prem deployment | Runs entirely inside the operator's Kuwait data centre; no patient data leaves the perimeter; air-gap-capable. |
| 2 | Kuwait Data Privacy Protection Regulation alignment | Documented mapping to CITRA-issued obligations; consent capture; retention controls; access log per encounter. |
| 3 | Bilingual EN+AR baseline | Full RTL framework support across kiosk, signage, SMS, web, console, PDF. Not a translation layer. |
| 4 | HL7 v2 integration | ADT (admission/discharge/transfer), order, and result messages; tested against the operator's HL7 gateway. |
| 5 | FHIR R4 endpoints | Modern REST APIs for Appointment, Encounter, Patient, Schedule resources. |
| 6 | DICOM-friendly imaging-clinic flow | Queue model handles imaging modalities (CT, MRI, ultrasound, X-ray) and reading-room routing. |
| 7 | Multi-site, multi-tenant | One head-office tenant, N clinic tenants; per-site config of hours, services, panels, holidays. |
| 8 | Virtual queueing | SMS / WhatsApp / web-based patient ticket; leave-and-return UX; ETA accuracy. |
| 9 | Online appointment | Self-service web booking; clinician-panel awareness; double-booking prevention; cancellation flow. |
| 10 | Wayfinding integration | Bilingual indoor wayfinding to consulting rooms; consistent with QMS call-forward IDs. |
| 11 | Customer feedback at the right moment | Post-encounter capture via SMS or kiosk; CSAT and NPS dashboards; routing to operations lead. |
| 12 | On-premises AI Clinical Assistant option | Open-weight LLM running on operator hardware; never sends PHI to a third-party API. |
| 13 | Audit + observability | Tamper-evident audit log of every ticket, call, no-show, and admin action; dashboards. |
| 14 | Fixed-fee phased delivery with exit | Discovery fixed-fee; Build milestone-fixed; 90-day exit window; operator owns the repo at the end. |
Three of the trickier criteria are worth unpacking.
Criterion 6 (DICOM-friendly imaging flow). Outpatient queues are not symmetric. Radiology has a different rhythm — patients arrive, change, wait for the modality, get scanned, then leave; the scan is read asynchronously. The QMS must model the modality as a service and respect the reading-room queue separately. Vendors that only model "counter A serves customer" fail here.
Criterion 12 (on-premises AI). 2026 procurement specs increasingly ask for an AI Clinical Assistant capability — pre-visit summarisation, intake triage, post-visit note drafting. The only safe pattern is running the model on the operator's own GPU hardware via vLLM, Ollama, or TGI, with open-weight models like Llama 3, Mistral, or Qwen. Anything that sends PHI to a hosted third-party API fails CITRA's data-residency expectations.
Criterion 14 (fixed-fee with exit). Time-and-materials with a foreign vendor is a procurement red flag. Insist on Discovery fixed-fee, Build milestone-fixed with weekly demos, change-orders priced before they start, and a 90-day exit window. That is how Zeour structures every engagement — including the MoH Kuwait deployment.
How do you choose between on-premises, sovereign cloud, and public-cloud SaaS in Kuwait?
Three deployment options surface in every Kuwait healthcare QMS RFP. They differ on cost, control, and CITRA-fit.
Option A — Sovereign on-premises. Servers in the operator's data centre, inside Kuwait. PHI never leaves the perimeter. This is the default for MoH-aligned providers and large private hospital groups. Higher capex on day one, but the only model that gives full control over patient data, integration to legacy clinical systems on the same network segment, and air-gap capability when a security incident requires it.
Option B — Sovereign cloud. A regional or Kuwait-hosted cloud tenancy under Kuwait jurisdiction. Less capex, faster initial deployment, but you trade some control. Acceptable for non-PHI surfaces — public-information signage, marketing analytics, anonymised dashboards.
Option C — Public-cloud SaaS hosted outside Kuwait. Cheapest sticker price. Hardest fit for PHI under the Kuwait Data Privacy Protection Regulation, because data leaves Kuwait and the operator loses jurisdictional control. Almost always ruled out for patient-data-touching surfaces.
The Zeour pattern across the region is sovereign on-prem for the PHI-bearing core, with an optional sovereign-cloud layer for non-PHI dashboards and a public web layer that proxies through the on-prem tenant without ever caching patient data.
> Procurement call-out. If your RFP scorecard does not allocate at least 25% of total marks to deployment topology, data residency, and exit ownership, you are about to commission a project that wins on demo quality and loses on year-three audit. Re-weight before issuing.
How much does healthcare queue management cost in Kuwait in 2026?
Sticker price is misleading without scope. The framework below is what experienced Kuwait healthcare buyers use.
| Phase | Scope | Indicative £ band (Kuwait market) |
|---|---|---|
| Discovery | 2-4 week scoping, integration map, clinical-flow workshops, written specification | £15k-£40k |
| Build (small) | Single hospital outpatient or 4-12 primary-care centres; queue + appointment + signage + customer feedback; integration to one EMR | £80k-£250k |
| Build (enterprise) | MoH-scale or large hospital group rollout; multi-site primary-care + hospital outpatient; full clinical workflow; on-premises AI option | £300k-£1M |
| Integration | Each clinical system (EMR, LIS, RIS-DICOM, pharmacy, identity gateway) | £20k-£80k per system |
| Per-site hardware | Counter terminals, kiosk, bilingual signage screens, networking | £8k-£25k per site |
| Care Plan (annual) | Monitoring, security patching, version updates, content updates, second-line support | 18-22% of Build |
Discovery is quoted in £; the contract is re-priced in local currency at signature with a defined adjustment window. See Zeour pricing for the wider commercial framework applying across UK, EU, Americas, GCC, MENA, Africa, and Asia.
Two cost levers matter.
Lever 1 — modularity. A QMS-only programme is the cheapest entry point. Adding online appointments, virtual queueing, wayfinding, and customer feedback each adds 15-30% to Build cost but compounds operational return. The most common Kuwait Build bundles queue + appointment + signage + feedback together — the configuration that moves the patient-experience needle on a board paper.
Lever 2 — integration count. Each external system adds a fixed cost. A pragmatic Kuwait Build integrates one EMR, one identity gateway, and one SMS or WhatsApp gateway on day one, sequencing LIS and RIS-DICOM into phase two. Landing all five in phase one is the most common reason a project slips go-live.
ROI calculator — build a defensible business case in 7 steps
The framework Zeour walks through during Discovery. Output is a one-page board-grade business case.
- 1Baseline wait time. Measure average and 90th-percentile wait time across primary-care centres or outpatient clinics today, per service. Most Kuwait sites without modern QMS sit at 45-90 minutes for primary care, 60-120 minutes for specialty outpatient.
- 2Baseline walk-away rate. Count patients who left without being seen, per day per site, over the last 90 days. A walk-away is a lost encounter, lost revenue, and a CSAT hit.
- 3Baseline no-show rate. Pull 90 days of booked appointments and divide no-shows by bookings. Kuwait primary-care baselines often sit at 18-25% without reminder discipline.
- 4Target uplift. Realistic post-Build: wait time down 30-45%, walk-away rate down 50-70%, no-show down 30-40% with reminder and easy reschedule.
- 5Direct revenue impact. Multiply recovered encounters by average encounter revenue. For a centre seeing 200 patients/day, recovering 5% is 10 extra encounters per day.
- 6Indirect impact. Improved CSAT and NPS via feedback capture; staff time freed; reduced complaints; improved board reporting.
- 7Total cost of ownership. Build + Care Plan + hardware over five years. A typical Kuwait multi-site primary-care Build pays back in 14-24 months on direct revenue alone.
For a worked example, the hospital outpatient digital front door playbook walks through a 6-site scenario; the same pattern applies to a Kuwait private hospital group.
Seven failure modes from Kuwait deployments
From Zeour's own delivery experience and observation of failed projects in the wider region.
1. Translating English UI into Arabic instead of bilingual at the framework layer. Symptom: RTL text rendered LTR, mirrored icons missing, Arabic numerals not flowing into PDFs. Fix: insist on bilingual baseline at the framework layer.
2. Buying public-cloud SaaS for PHI workflows. Symptom: stalled CITRA security review, procurement officer escalating to the CISO. Fix: sovereign on-prem for the PHI-bearing core.
3. Integrating to the EMR after go-live, not before. Symptom: duplicate patient identifiers, reconciliation work that grows monthly. Fix: HL7 v2 ADT integration is phase-one mandatory.
4. Under-modelling the imaging-clinic flow. Symptom: radiology queue piles up because the QMS models the CT scanner as a counter. Fix: model DICOM modalities and reading-room flow during Discovery.
5. Under-investing in the call-forward console. Symptom: clinicians refuse to use the QMS because it adds clicks. Fix: usability-test the console with three clinicians during Discovery and adjust before Build.
6. Neglecting feedback capture. Symptom: operations director cannot prove CSAT improvement. Fix: bundle feedback capture at the right moment — typically SMS within two hours of discharge.
7. Buying time-and-materials from a foreign vendor. Symptom: scope drift and 50% over budget by year two. Fix: insist on fixed-fee phased delivery with a 90-day exit window and operator-owned source code — how the MoH Kuwait engagement was structured.
Migration path
If you already have a legacy QMS — typically a ticket dispenser plus a single reception screen — here is the migration sequence Zeour follows.
Week 0-2: Discovery. Site walks at two representative clinics, EMR vendor conversation, integration map, written specification, success metrics signed off. Output is a 30-40 page spec and Build SOW.
Week 3-10: Build (parallel). New platform installed sovereign on-prem alongside legacy. Bilingual UI at framework layer. HL7 v2 ADT integration against a test EMR feed. Virtual queueing and online appointment delivered. Feedback capture wired.
Week 11-14: Pilot at two sites. Run new platform in parallel with legacy at one primary-care centre and one specialty outpatient clinic. Measure wait time, walk-away rate, no-show rate, and feedback against baseline.
Week 15-22: Phased rollout. Two to four sites per week. Legacy decommissioned per site as new platform stabilises. Care Plan begins per site at go-live.
Week 23-26: Stabilisation and handover. Operator team trained, runbooks signed off, Care Plan activated, exit window confirmed. Operator owns source code, deployment scripts, and license keys.
Migration runs 6 months for a multi-site primary-care or single-hospital deployment. Enterprise programmes with phase-two integrations and on-premises AI run 9-12 months.
Implementation playbook
Five workstreams run in parallel through Build.
Clinical flow design. Map the patient journey for each service type, end to end. Identify pre-arrival, check-in, waiting, consultation, post-visit, and feedback touchpoints. Specify which surface owns each step — kiosk, console, signage, SMS. Lock in the bilingual baseline.
Integration engineering. Stand up an HL7 v2 gateway against the operator's EMR. Build FHIR R4 endpoints for Appointment, Encounter, Patient, and Schedule resources. Wire the identity gateway and SMS / WhatsApp gateway. Test against synthetic patient data.
Hardware deployment. Specify counter terminals, kiosks, bilingual signage, network drops, and UPS per site. Source through Kuwait-resident hardware partners where possible. Stage centrally before per-site install.
On-premises AI (optional). If the operator opts into the AI Clinical Assistant, specify GPU hardware, deploy the inference stack (vLLM, Ollama, or TGI), load an open-weight model (Llama 3, Mistral, or Qwen), build the RAG pipeline, and define mode-based prompts. No PHI leaves the perimeter.
Change management. Train reception staff, clinicians, and operations leads. Build runbooks for incident response, security patching, content updates, and backup verification. Hand to the operator's IT team in week 23 with sign-off from both sides.
The deliverable at week 26 is a sovereign, bilingual, fully integrated, audit-ready patient-flow platform the operator owns end-to-end.
Frequently asked questions
Does the Kuwait Data Privacy Protection Regulation require on-premises hosting for patient data?
The regulation does not literally mandate on-premises; it mandates control, consent, retention, and breach-notification obligations that are easier to meet on infrastructure the operator runs inside Kuwait. The defensible posture is sovereign on-prem for PHI; sovereign cloud is acceptable for non-PHI surfaces.
Is bilingual EN+AR a real procurement requirement in Kuwait healthcare?
Yes. Every patient-facing surface — ticket, kiosk, signage, SMS, web, console, PDF — has to render correctly in English and Arabic with full right-to-left support. Score this at the framework layer.
Can Zeour integrate with our existing EMR via HL7 v2?
Yes. HL7 v2 ADT, orders, and results are baseline for every Zeour healthcare deployment, with FHIR R4 endpoints for modern integrations.
How does the platform handle imaging clinics with DICOM modalities?
The queue model represents each modality as a distinct service with its own panel, capacity, and reading-room workflow. DICOM integration is scoped during Discovery against the operator's existing PACS and modality worklist setup.
Does the AI Clinical Assistant send patient data to a third-party API?
No. The AI Clinical Assistant runs on the operator's own GPU hardware using open-weight models, with the inference stack inside the operator's perimeter. PHI never leaves the operator's infrastructure — the only posture compatible with the Kuwait Data Privacy Protection Regulation.
Can we run telemedicine on the same platform?
Yes. The clinic management platform ships with a WebRTC telemedicine capability for video consultations, integrated into the same patient identity, appointment, and queue model.
What does the 90-day exit window actually mean?
At the end of any phase, the operator has 90 days in which Zeour hands over source code, deployment scripts, license keys, runbooks, and architecture documentation. The operator can take the system in-house, transition to a different partner, or continue with Zeour's Care Plan.
How does this compare to a typical KSA healthcare deployment?
The regulatory frame differs (CITRA in Kuwait, SDAIA and NCA in KSA) and integration patterns vary, but the architectural posture is identical: sovereign on-prem, bilingual baseline, HL7 / FHIR / DICOM integration, fixed-fee phased delivery. The KSA healthcare buyer's guide walks the parallel framework.
How do you handle Kuwait Vision 2035 alignment in a procurement narrative?
Kuwait Vision 2035 prioritises citizen-experience digital services and a modernised healthcare system. A QMS programme delivers patient-experience uplift, reduces wait times, and improves operational reporting — all mapping directly to the Health pillar.
What does a first conversation with Zeour look like?
A 45-minute call to walk through your site list, your existing systems, your bilingual + sovereign expectations, and your timeline. If the fit is there, we send a Discovery SOW within five working days.
Where Zeour fits
Zeour Ltd is a UK-registered company shipping a 12-solution enterprise platform worldwide — across UK, EU, Americas, GCC, MENA, Africa, and Asia. Our queue management ecosystem is in production at 1,247+ branches across 40+ countries; the MoH Kuwait engagement proves the model in the Kuwait healthcare context.
For a Kuwait healthcare buyer, the relevant pieces of the platform are the queue system for in-clinic patient flow, virtual queueing for leave-and-return UX, the online appointment system for self-service booking, the MediCare clinic management system for full EMR + AI Clinical Assistant + telemedicine, wayfinding for bilingual indoor navigation, and customer feedback for measurable CSAT uplift. The bilingual on-prem clinic management guide goes deeper on the clinical-system layer.
The delivery model is consistent: sovereign on-premises by default, bilingual EN+AR as a production baseline with any other locale added per engagement, fixed-fee phased delivery, weekly demos, change-orders priced before they start, a 90-day exit window, and operator ownership of the repo and license at the end. The optional on-premises AI layer runs on the operator's hardware using open-weight models — no PHI ever leaves the perimeter.
If you are sizing a 2026 programme, the healthcare industry page is the right place to start; the contact page is the right place to finish. We will reply within one working day with a Discovery SOW shaped to your site list, your existing clinical-systems stack, and your Kuwait Vision 2035 alignment narrative.
---
Zeour Ltd — sovereign enterprise software shipped worldwide. UK-registered, delivered everywhere.